2018년 9월 28일 금요일
[CCTR 692] -0921- Ethical issue(informed consent)
0921
I. NIH/FDA guidance's for inclusion of minority(race, ethnic subgroup)
In Phase III Clinical Study(several hundred - efficacy test)
Sex(Woman, minority)
Ethnicity & Race(Hispanic -> Hawaiian, More than one race)
II. Ethical issue
Without impairing the warfare of individuals.
- Minimize ?harm
- No serious harm(stop)
- value, scientific validity, fair selection, favorable benefit, risk balance, independent review,
informed consent, respect participants.
- Protection from conflict interest(financial, intellectual): minimize bias.
III. Informed consent
let them know the information clearly.
- Nurenberg Code 1947(1st)
- Declaration of Helsinki(1964 ~ 1996); international ethics/rules
- Belmont Report 1979; respect for person, beneficence, justice
Part of informed consent; A process + A document(informed sheet, consent form with signature)
IV. Integrity
Sharing data <-> Confidentiality.
Data falsification.
2018년 9월 27일 목요일
[ ] [CK] Fat pad biopsy for amyloidosis
- Endomyocardial Biopsy results negative for Amyloyd
- However PYP scan completed 9/25 - results + for TTR cardiac amyloidosis
- Genetic testing obtained 9/25 - also pending
- Fat Pad Biopsy scheduled for 12:30 pm in Non-Vasc Lab om 9/27
- No Heparin gtt 1.5 to 2 hrs prior to bx
Cardiac Bx
PYP Scan
Fat Pad Bx.
- However PYP scan completed 9/25 - results + for TTR cardiac amyloidosis
- Genetic testing obtained 9/25 - also pending
- Fat Pad Biopsy scheduled for 12:30 pm in Non-Vasc Lab om 9/27
- No Heparin gtt 1.5 to 2 hrs prior to bx
Cardiac Bx
PYP Scan
Fat Pad Bx.
[CK] Vancomycin trough(prior to 30mins to 1 hr) - RENAL
1.You should check prior to the 4th or 5th dose.
2. Initial/change dose -> recheck every 4th dose but if you really concern, can check even earlier with discussion with pharmacy.
3.Renal function change/UOP change/nephrotoxic meds => recheck
4.Long term => once a week check
[CK] Cocaine induced chest pain or MI(ACS) in setting of cocaine abuse
Rule of thumb
1. MI : GO GIVE B-blocker !!(METOPROLOL!) Save the heart first
2. Others: Can go with NTG/CCB + labetalol / carvedilol.
Avoid esmolol, propranolol, metoprolol alone(long term or low risk CP)
1. MI : GO GIVE B-blocker !!(METOPROLOL!) Save the heart first
2. Others: Can go with NTG/CCB + labetalol / carvedilol.
Avoid esmolol, propranolol, metoprolol alone(long term or low risk CP)
2018년 9월 26일 수요일
[CK] ACT vs PTT to pull sheath out.

PTT 30-50: WNL
ACT 99-130: WNL
So Remove sheath ACT < 170(arterial) or < 200(venous access) or <150(PCI)
PTT < 60(50)
https://www.sciencedirect.com/topics/medicine-and-dentistry/sheath-removal
[ ] [CK] ICD/ PM interrogation.
<UW> -basic interrogation for Fellow
<Uptodate>
https://www.uptodate.com/contents/cardiac-implantable-electronic-devices-patient-follow-up
<ICD PM basic in clevland clinic>
https://my.clevelandclinic.org/ccf/media/Files/nursing/2014-dicc-handouts/Session9_1030_1103_Donatello.pdf
<ACC guideline>
https://www.acc.org/~/media/Non-Clinical/Files-PDFs-Excel-MS-Word-etc/Meetings/2016/Course%20PDFs/Core%20Curriculum/Friday/Fri%207%2030%20am%20Obias-Manno%20pdfp.pdf
<Trouble shooting>
http://www.bhrs.com/files/files/How%20To%20%26%20Techniques/140814-Education,%20ICD%20Troubleshooting.pdf
<Medtronic guide>
https://www.medtronic.com/content/dam/medtronic-com/global/HCP/Documents/reportinpace-rev.pdf
~ UW:
<Uptodate>
https://www.uptodate.com/contents/cardiac-implantable-electronic-devices-patient-follow-up
<ICD PM basic in clevland clinic>
https://my.clevelandclinic.org/ccf/media/Files/nursing/2014-dicc-handouts/Session9_1030_1103_Donatello.pdf
<ACC guideline>
https://www.acc.org/~/media/Non-Clinical/Files-PDFs-Excel-MS-Word-etc/Meetings/2016/Course%20PDFs/Core%20Curriculum/Friday/Fri%207%2030%20am%20Obias-Manno%20pdfp.pdf
<Trouble shooting>
http://www.bhrs.com/files/files/How%20To%20%26%20Techniques/140814-Education,%20ICD%20Troubleshooting.pdf
<Medtronic guide>
https://www.medtronic.com/content/dam/medtronic-com/global/HCP/Documents/reportinpace-rev.pdf
~ UW:
PACEMAKER AND ICD BASICS.
PERI-IMPLANTATION MANAGEMENT
Pre-op: Assess for bleeding diathesis (platelets <50) – many patients are on coumadin and this is ok as long as they are within the range that is therapeutic for their indication. Touch base with individual attendings if concern and they are anticoagulated for planning purposes. If patient has had lines/procedures/devices before in the left subclavian, consider getting an upper extremity U/S to assess venous access. Look for any sign of infection, ask for U/A, blood cx’s, cxr if there is any question. The patient should not have a central line on the side where the device is to be implanted, and preferably has a peripheral IV on the side in case a venogram is needed. Pre-op orders are typically written by the 3rd/4th year EP fellows, but include: NPO after MN, Heparin gtt off at 4am, Cefazolin 2g IV & Cefazolin flush 1g in 500cc NS (or Vancomycin 1g IV & Vanco flush 1g in 500cc NS) on call to EP lab. Post-op: Wound check the morning after and in one week (usually as an outpatient). PA & Lateral CXR on the morning after procedure. NO LOVENOX. IV Heparin is usually OK the next morning, no bolus, but check with the attending. Any sign of bleeding into the pocket should be prompt a discussion with the attending. Check with EP fellow if any questions. They are expected to do the post op care unless they speak to you.
Device infections: If a patient comes to the ED with a device that is eroding through the skin, has a wound dehiscence, or pus at the site, they needed to be admitted. Devices that are infected need to come out, leads and all. Talk to the EP attending if there are any questions.
INTERROGATION BASICS
- When you get called to interrogate a device, ask the primary service to identify the type of device they have. (Medtronic, Guidant/Boston Scientific, St. Jude, Biotronik, and ELA are the 5 companies whose devices we are able to interrogate. For others, you will have to call the rep directly.)
- You must have the proper programmer (device interrogation machines) to perform an interrogation. (e.g. The Medtronic programmer will not work on a Guidant device). Programmers can be found on 5NE, but also in the EP lab or cardiology clinic. Don’t forget to take extra paper and ECG leads for the programmer.
- You should always feel safe interrogating a device. Print out everything you see and if you have any questions, you can go over it with an attending later. If you are uncomfortable reprogramming a device, go over your interrogation with someone first, then go back and reprogram the device later.
A basic note of a complete, standard interrogation of a pacemaker or ICD should include:
1. Device & manufacturer
2. Current Battery Voltage (note ERI voltage as well)
3. Last Full Energy Charge Time for ICD’s (< 15 seconds is normal)
4. Leads (The device will measure impedance, you need to check thresholds and usually sensing)
a. Impedance (300-1000 Ohms is normal, except in high-impedance leads)
b. Sensing (Normal: A > 1mV, V > 5mV.)
c. Threshold (Ideally: Atrium: 1V @ 0.4ms or less, Ventricle: 1-2V @ 0.4ms or less)
5. Percent of time paced and sensed in A and V
6. Underlying rhythm (test this by decreasing the pacing rate sequentially until no longer pacing or by temporarily suspending pacing)
7. Mode Switch Episodes for pacemakers (e.g. “none”, “3”, “frequent”, “in progress”)
8. Tachy events for ICD’s
9. Sensing threshold setting (normal <1/2 sensing capability)
10. Pacing Output (should be set at twice the pacing threshold for voltage, three times threshold for pulse duration)
WHAT TO DO WHEN AN ICD FIRES:
(updated 8/2014)
Patients have been instructed to seek medical attention at the very first time the ICD fires. Most of them will come into the ER or you may get called by the patient directly overnight if you are on CB/EP call or Triple call:
- If it is a single firing and the patient feels otherwise well, have them CALL the clinic in the AM (or Monday AM if it is a weekend) to address f/u. If they have a home transmission kit, have them connect and send a transmission as well.
- If they have persistant chest pain suggestive of an MI, worsening HF symptoms or dizziness they need to come into the ER/call 911. If multiple shocks have gone off, the patient should also come into the ED.
- A routine evaluation should be performed by the ER, including labs and CXR. You should come in to assess the patient and interrogate the device to assess for arrhythmia or device malfunction. This may represent a VT storm and requires an admission to rule out ischemia and assess for causes of increased arrhythmias.
- The EP attending must be called if you do an interrogation in the ED to help decide if an admission is needed or any further suggestions/programming changes/medical management decisions.
BEING CALLED TO THE OR FOR PACEMAKERS AND ICDS
The main issue in the OR is that a PM/will detect electrocautery and interpret it as a native QRS complex and inhibit pacing inappropriately and an ICD could shock for mistaken VT/VF. If there is no electrocautery being used, it is safer to do NOTHING (no reprogramming, no magnet). Surgeries far from the device (i.e. ankle surgery) are unlikely to be detected by the device. For most surgeries here are your options:
For PM’s first find out if the patient is PM dependent. You may be able to find this in ORCA but you probably should interrogate the device first (the calling MD will NOT be able to tell you). If the patient is PCM dependent there are 3 options:
a. Use a magnet which will put the PCM to a VOO or DOO (asynchronous) mode. (This is acceptable in 90% of cases, but anesthesiologists hate it.)
b. Program the PCM to a VOO/DOO mode. (If OR field does not allow for secure taping of the magnet.)
c. Advise the OR to use cautery for no more than 2-3 seconds at a time to limit asystole. (Usually in emergency cases where there is not time to reprogram.)
d. Keep in mind, you are not doing non-pacemaker-dependent patients a favor by changing their device to VOO/DOO. It introduces a (very small) chance of pacing on the T wave and inducing polymorphic VT, they may also lose AV synchrony, and they probably have an increased risk of AF. Anesthesia rarely understands this but will usually listen to you if you talk to them rationally. Many anesthesiologists want the pacing rate increased to 70-80BPM.
Ask them.
For ICD’s, if there is cautery use, you need to come in to turn them off. In emergent cases, it is OK to just use a magnet which will turn the VT/VF therapy off but will not affect the pacing mode of an ICD. Keep in mind, the device companies generally recommend using a magnet for surgery, but UW anesthesia insists on devices being reprogrammed. To turn the ICD shock therapy off:
1. Print out the original settings before you change anything.
2. Under “Tachy Therapies” go to Detection. Turn the detection mode to “Off” for VT and then VF, in that order. This is the easiest way to “turn the ICD off” during surgeries because it preserves all the therapy settings.
3. Advise the OR to place defibrillator pads during the surgery and that the patient must remain on tele until the device is reprogrammed.
4. Remember that the bradycardia pacing mode is still on. If the patient is also pacemaker dependent, electrocautery may cause interference and you should program this to VOO/DOO. This is done under “Brady Therapies”. VOO/DOO is NOT an option in some devices, so if you can’t find it, don’t be surprised. Talk to an EP attending on-call if there is any question.
5. After surgery, perform a full interrogation and turn the ICD back on by programming the “Detection” back to the way it was set before. If the patient comes out of the OR in the middle of the night, it is worth checking the next day to make sure someone got called to turn the device back on.
TRANSVENOUS PACEMAKERS
Temporary transvenous pacemakers should be placed in the cath lab using fluoroscopy if at all possible, though often it’s not. There are multiple slight variations on this, here’s the general technique. Start by placing the correct sheath in right IJ or L subclavian (check the particular pacing wire you have first for what size sheath you will need – it is generally a 5 F sheath and all in the kit – larger ones will leak), don’t forget the swan-dom and then place the wire into the mid-floor to apex of the RV. When the wire is in the mid-floor of the RV, deflate the balloon, advance the wire 2-3mm more under fluoroscopy, and then hook up the pacemaker generator. Then follow the steps below to set up the generator properly below.
If you are floating a temporary wire without fluoroscopy, hook the wire up to the generator before you put it through the sheath. After the wire is through the sheath, inflate the balloon the way you would a Swan-Ganz catheter and turn the pacemaker on. Pace at a rate faster than the native intrinsic heart rate and at 20mA of output. Advance the wire until capture, approximately 20-30cm until fairly consistent capture is seen. Deflate the balloon and advance the wire just 1-3mm further. Slowly turn down the output to 5mA and follow the steps below. In emergent situations, have the primary service place the 5F sheath as you are driving in – this may save you a lot of time in the middle of the night. Just be sure to clean it with chlorhexidine before you put the wire in.
1. Set the rate 10-20 beats faster than the intrinsic heart rate (or at least 60bpm) and set the output to 5mA.
}2. Reposition the lead if needed until it captures at 5mA.
}3. Determine the Pacing Threshold:
a. Turn down the output until you first lose capture, this is the pacing threshold. Ideally, the pacing threshold should be < 1mA if the pacing wire is in good position. If the pacing threshold is above 3mA, it should generally be repositioned.
b. After you find the pacing threshold, raise the output back up to a safety margin of 3 times the pacing threshold or at least 3mA and leave it there.
4. If VVI pacing is desired (not always necessary), determine the Sensing Threshold:
a. Turn the pacemaker to VVI and the sensitivity to zero. The pacemaker should sense every beat and probably other artifactual ECG finding and fire rarely.
b. Slowly turn up the mV for sensing until asynchronous pacing is seen (this decreases the sensitivity for detecting native electrical activity). This is the sensing threshold.
c. Turn the mV back down to about half of the sensing threshold, or in other words: set the pacemaker to sense at “twice” the sensing threshold. The pacemaker should sense only real beats and not artifact (oversensing).
- Check the pacing and sensing threshold on all temporary pacemakers daily. It is common to find that the pacing threshold slowly increases each day due to inflammation at the contact point, slight malposition or thrombus on the pacing lead. If left in long enough, the pacing threshold will eventually become unacceptably high and a new pacemaker (preferably a permanent one) will need to be placed.
- Occasionally we place active fixation (a.k.a. “screw-in leads”) leads in the cath lab. It’s better to just see this than read about it. If you are called by another service and asked ‘How do you pull a temporary pacemaker’, make sure you know if it was a screw-in lead before telling them to just pull it. You should probably pull it though, just for safety.
- Epicardial pacemaker leads use the same type of generator as transvenous pacemakers and are adjusted the same way with essentially the same goals for threshold values. If you note increasing capture thresholds on epicardial leads, beware they tend to rise exponentially. So by the time they hit the high teens they’ll probably fail to capture within 24 hours, depending on the situation. You do not need to check threshold on temporary epicardial wires.
ROUTINE POST OP CIED IMPLANTATION CARE
· Check telemetry and am ECG for signs of arrhythmia or pacemaker malfunction
· Remove arm sling and discard
· Remove primapore dressing and check for intact incision, r/o hematoma.
· Examine patient including
o Lungs and heart for signs of PTX or effusion
o PM pocket for signs of hematoma or dehiscence
§ If hematoma, contact attending and consider a pressure dressing
· Check AM two view CXR (should come back by 9am) to evaluate
o Lead position (should be similar to the post-op AP)
o Generator position
o Proximal leads are fully deployed beyond set screw
o r/u ptx, hemothorax, enlarging cardiac silhouette etc.
· Device will be interrogated by the device company (weekend) or by the clinic nurses (8 3795 if weekday) and the numbers emailed to the on-call attending or placed in chart or ORCA (nurses).
· Ensure Pain control is adequate
· Ensure scripts are written for antibiotics post-implant if needed (based on implanting attending and circumstances of the case – usually 3 days).
o Keflex, unless PCN allergic, then doxycyline
· Ensure instructions for post-pacemaker or post-ICD care are included in discharge paperwork
· Restrictions
o Keep wound dry for 48 hrs
o No soaking wound or immersing in water for 2 wks
o Lifting restrictions for any new lead is <10lbs for 30 days with the ipsilateral arm
o We prohibit abduction of the ipsilateral arm above 90 degrees for 30 days (so up to shoulder is ok)
· The EP lab will arrange for follow-up for wound check and device check in 10days-2wks or so
o Check visits and put this information in discharge paperwork if it has been scheduled (f/u is scheduled by Natalie preoperatively, but may not be correct for patients followed outside of UWMC)
o If not yet scheduled, notify patient we will contact them to arrange follow-up and if they do not hear from anyone to call the EP department in the next few days to arrange follow-up
· Once the above are completed, touch base with on-call attending to make sure no other clinical issues are outstanding and discharge.
ROUTINE POST-ABLATION (ATRIAL FIBRILLATION, ATRIAL FLUTTER, SVT) CARE
· Most patients go home post-op day 1, however prior to this, need to:
o Check telemetry and ECG for signs of arrhythmia or changes in rhythm
o Examine patient, specifically lungs and heart as well as groins and limbs to ensure hemostasis and distal circulation
o Confirm antiarrhythmic/AV nodal agent plan with attending if unclear from operative note or post-operative notes
[CK] mixed venous saturation.
Normal values of mixed venous oxygen saturation (SvO2) are 60 - 80%. Central venous oxygen saturation (ScvO2) values represent regional venous saturations with a normal value of ~70%. ScvO2 usually measures slightly higher than SvO2 as it has not mixed with the venous blood from the coronary sinus.
SVO2: >60%(60-80) with coronary sinus
ScvO2(Internal jugular, or subclavian without coronary sinus = venous blood from heart => lowered than general average): 70%
SVO2: >60%(60-80) with coronary sinus
ScvO2(Internal jugular, or subclavian without coronary sinus = venous blood from heart => lowered than general average): 70%
2018년 9월 25일 화요일
[CK] Long RP vs Short RP (RP vs PR, if it's longer = long RP, shorter = short RP)

Mostly long RP = A- tach or S- tachy
Short RP = most of SVT (if it's much shorter <70 = AVNRT vs relatively longer >70 but short.= AVRT)

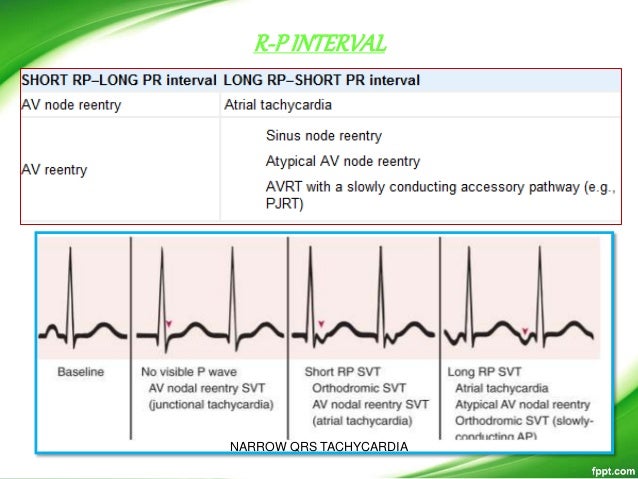
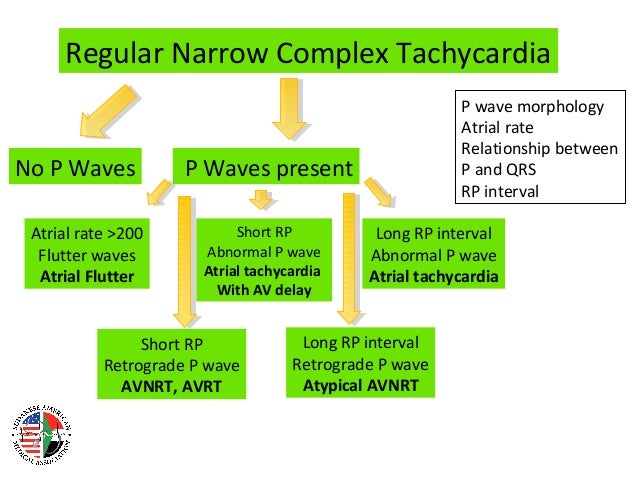
no P = AVNRT(junctional)
P(sawtooth or >200) = A flutter
Long vs Short(less than half or more than half)
Long RP = Atach, Sinus tach. <= abnormal but not retro P. cf) if it's retro P <= atypical SVT(AVNRT
Short RP = AVNRT(<70), AVRT(>70), retro P <= reentry SVT(for sure!)
Aflutter
Typical: Sawtooth. From Rt. TV Isthmus
Atypical: No Sawtooth. Not from RA. Isthmus.
[CK] R/O Malingering in patient's lt. leg weakness. Hoover's test and Abductor test.
Hoover's test:
Cup heels and
raise opposite limb
True paresis if no difference in downward pressure at heels.
Abductor:
Ask patient to abduct paralytic leg to resistance.
True paresis if opposite leg abduct only.
Cup heels and
raise opposite limb
True paresis if no difference in downward pressure at heels.
Abductor:
Ask patient to abduct paralytic leg to resistance.
True paresis if opposite leg abduct only.
2018년 9월 24일 월요일
[CK] VT morphology(Ventricular tachycardiac vs others) reciting = wall




<diss, RS>
1) AV dissociation = 100%
2) RS > 100 = 100%
3) No RS = 100%
<qwave or marriot in v1 or v6>
<qwave or marriot in v1 or v6>
4) non typical LBBB, RBBB in both v1, v6 = 100%
LBBB(V6) = Q in V6
RBBB(V1) = Q in V1, MONO, BIG Lt. year in v1(Marrioit sign)
<3= joseph slow axis!>
5) Nadir(notch = Josephs sign)
6) feature: slow -> quick (slow slow quick quick!! why? : ) SLOW = VT.
=NOTCH WITH SLURRING = VT.
7) Extreme axis: POSITIVE IN avR!!!(NEGATIVE IN avL => Totally NORTHWEST= RT!!)
7) Extreme axis: POSITIVE IN avR!!!(NEGATIVE IN avL => Totally NORTHWEST= RT!!)
[CK] Symptomatic or frequent NSVT - needed to be treated with BB and AAD
For some patients who have
frequent, (frequent VPBs (median frequency 18 per hour) = 18 PVC in HR = needed to be treated.=> NSVT = )
highly symptomatic NSVT
not adequately suppressed by beta blockers or calcium channel blockers, the addition of antiarrhythmic medications (table 1) may be helpful.
We suggest amiodarone as the initial choice, rather than other antiarrhythmic drugs, based on its efficacy (Grade 2C). (See 'Antiarrhythmic drugs' above.)
frequent, (frequent VPBs (median frequency 18 per hour) = 18 PVC in HR = needed to be treated.=> NSVT = )
highly symptomatic NSVT
not adequately suppressed by beta blockers or calcium channel blockers, the addition of antiarrhythmic medications (table 1) may be helpful.
We suggest amiodarone as the initial choice, rather than other antiarrhythmic drugs, based on its efficacy (Grade 2C). (See 'Antiarrhythmic drugs' above.)
[CK] POTS Postural tachycardia syndrome.
Dx. head-up tilt testing: HR > +30 over baseline or to >120 bpm.
Dx. of exclusion: Dehydration, prolonged bedrest, medications, and other dysautonomia
Tx. not established. Same as orthostatic hypotension.
[CK] Kidney stone 1) tamsulosin, 2) +- nifedipine or tadalafil or sildosin. 3) pain control: NSAID, analgesic.
In addition to tamsulosin and nifedipine, tadalafil and silodosin can be used as MET [117,118]. In a trial, 285 patients with distal ureteral stones sized 5 to 10 mm in diameter were randomly assigned to tamsulosin (0.4 mg/day), silodosin (8 mg/day), or tadalafil (10 mg/day) until stone passage or for a maximum of four weeks [118]. Silodosin resulted in significantly higher rates of stone expulsion (83 compared with 64 percent with tamsulosin and 67 percent with tadalafil) and significantly faster mean expulsion times (15 days versus 17 days with tamsulosin and 16 days with tadalafil). Additional studies are needed to evaluate the safety and efficacy of tadalafil and silodosin as MET.
International guidelines from the American Urological Association and the European Association of Urology on the management of ureteral calculi suggest that:
●"In a patient who has a newly diagnosed ureteral stone <10 mm and whose symptoms are controlled, observation with periodic evaluation is an option for initial treatment. Such patients may be offered an appropriate medical therapy to facilitate stone passage during the observation period. In a choice between active stone removal and conservative treatment with MET, it is important to take into account all individual circumstances that may affect treatment decisions. A prerequisite for MET is that the patient is reasonably comfortable with that therapeutic approach and that there is no obvious advantage of immediate active stone removal" [51,119].
Patients will typically require analgesics such as ketorolac. Concurrent antibiotics are used by some groups but have not been studied to determine their value in the setting of a patient receiving MET. Patients with stones larger than 10 mm in diameter, patients with significant discomfort, those with significant obstruction, or who have not passed the stone after four to six weeks should be referred to urology for potential intervention.
UROLOGY CONSULTATION — Urgent urologic consultation is warranted in patients with urosepsis, acute kidney injury, anuria, and/or unyielding pain, nausea, or vomiting [4,120]. Outpatient urology referral is indicated in patients with a stone >10 mm in diameter and in patients who fail to pass the stone after a trial of conservative management, including medical expulsive therapy (MET), particularly if the stone is >4 mm in diameter or if there is uncontrolled pain [87,121].
[R] Cohort study(Same sample) and Longitudinal study(New sampling)
Cohort studies are usually prospective longitudinal studies - i.e. they follow they same sample through multiple waves forward in time. Longitudinal studies can also be repeated cross-sectional studies, which involve collecting data from a new or largely new sample at multiple points in time. Longitudinal studies can also gather data on past events, which is a retrospective design.
[R] Data type. Categorical(frequency only) = Nominal or Ordinal, Numeric(0)

Categorical: Nominal -> Ordinal
Continuous: Numeric(Interval=no "0" -> Ratio=true "0")
2018년 9월 12일 수요일
[Q} [CK] Cardiac clearance.
https://www.uptodate.com/contents/evaluation-of-cardiac-risk-prior-to-noncardiac-surgery#H2
2018년 9월 10일 월요일
[CK] Colchicine - Renal impairment(higher concentration)
To date, no investigation has revealed the site of kidney lesion or dysfunction.
But not nephrotoxic.
GFR<10 then consider half dose. No contraindication in AKI.
But concerning with high level and side effect.
Avoid in hepatotoxicity.
But not nephrotoxic.
GFR<10 then consider half dose. No contraindication in AKI.
But concerning with high level and side effect.
Avoid in hepatotoxicity.
[CK] Physical examination
S4:
S4 is caused by stiffening of the walls of the ventricles (usually the left)
S4 is caused by stiffening of the walls of the ventricles (usually the left)
피드 구독하기:
글 (Atom)